
ISSUE1759
- Jean-Marie Pflomm, Pharm.D., Editor in Chief has disclosed no relevant financial relationships.
- Brinda M. Shah, Pharm.D., Consulting Editor has disclosed no relevant financial relationships.
- Review the efficacy and safety of ensitrelvir (Xocova) for post-exposure prophylaxis of COVID-19.
- Description: An oral SARS-CoV-2 main protease inhibitor
- Indication: Postexposure prophylaxis of COVID-19 in patients ≥12 years old who had contact with an infected individual
- Efficacy: In one clinical trial, a 5-day course of ensitrelvir reduced the incidence of laboratory-confirmed COVID-19, compared to placebo, in household contacts of an infected individual (relative risk 0.33).
- Adverse Effects: Most common were headache, diarrhea, cough, and decreased hemoglobin levels.
- Drug Interactions: Increases serum concentrations of drugs that are CYP3A substrates or are transported by P-gp or BCRP. Use of ensitrelvir with drugs that are primarily metabolized by CYP3A or with strong CYP3A inducers is contraindicated.
- Pregnancy and Lactation: Should not be used by pregnant or breastfeeding women
- Dosage: 375 mg PO on day 1 (taken within 72 hours of exposure), followed by 125 mg on days 2-5
- Cost: A 5-day course costs $1400.
- Conclusion: Ensitrelvir reduces the risk of COVID-19 in household contacts of an individual infected with SARS-CoV-2.
The FDA has approved ensitrelvir (Xocova – Shionogi), a SARS-CoV-2 main protease inhibitor, for postexposure prophylaxis of COVID-19 in patients ≥12 years old who had contact with an infected individual. Ensitrelvir is the first oral antiviral drug to be approved in the US for this indication. The parenteral monoclonal antibody combinations bamlanivimab and etesevimab and casirivimab and imdevimab (REGEN-COV) are no longer authorized for postexposure prophylaxis of COVID-19 in the US.

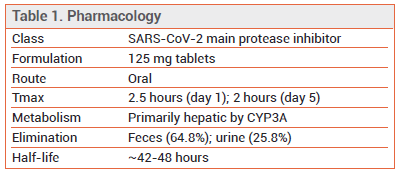
PHARMACOLOGY — Ensitrelvir inhibits SARS-CoV-2 3C-like protease, preventing viral replication.1,2 Because ensitrelvir targets a region of the SARS-CoV-2 virus that is highly conserved, the drug is expected to be effective even when the virus mutates and alters the antigenicity of the spike protein. Ensitrelvir treatment has been associated with 3CL protease substitutions that confer reduced susceptibility to the drug in vitro.3
CLINICAL STUDIES — Postexposure Prophylaxis – FDA approval of ensitrelvir was based on the results of a double-blind trial (SCORPIO-PEP) in 2041 household contacts ≥12 years old who were exposed to SARS-CoV-2 but tested negative for SARS-CoV-2 at baseline. Exposed patients were randomized to receive ensitrelvir or placebo once daily for 5 days, started within 72 hours of symptom onset in the index patient. The incidence of laboratory-confirmed COVID-19 within 10 days of treatment was significantly lower with ensitrelvir than with placebo (2.9% vs 9.0%, RR 0.33 [NNT 16.4]).4
Treatment – In one double-blind trial (SCORPIO-SR) in standard-risk adults with mild to moderate COVID-19, ensitrelvir started within 3 days of symptom onset reduced the time to resolution of a composite of 5 typical COVID-19 symptoms (stuffy or runny nose, sore throat, cough, feeling hot or feverish, low energy or tiredness) by one day compared to placebo.5 In another trial (SCORPIO-HR) in nonhospitalized adults with mild to moderate COVID-19 who were at standard or high risk for severe disease, ensitrelvir started with 3 days of symptom onset did not significantly reduce the time to complete resolution of all symptoms (a composite of 15 symptoms including loss of smell or taste) compared to placebo, but it did reduce viral load.6
ADVERSE EFFECTS — The most common adverse effects (frequency ≥1% and greater than with placebo) of ensitrelvir in clinical trials were headache, diarrhea, cough, and decreased hemoglobin levels. Transient decreases in high-density lipoprotein cholesterol (HDL-C) have been reported. Anaphylaxis, angioedema, and urticaria have occurred rarely with use of the drug in other countries.
DRUG INTERACTIONS — Ensitrelvir is a substrate of CYP3A and it inhibits CYP3A, P-glycoprotein (P-gp), and breast cancer resistance protein (BCRP). The drug can increase serum concentrations of drugs that are metabolized by CYP3A or transported by P-gp or BCRP. Coadministration of ensitrelvir and drugs metabolized primarily by CYP3A is contraindicated. Concurrent use with strong CYP3A inducers can reduce serum concentrations of ensitrelvir and is also contraindicated.7
PREGNANCY AND LACTATION — In studies in pregnant animals, administration of ensitrelvir was associated with skeletal malformations and embryofetal death. Females with reproductive potential should use effective contraception during treatment with ensitrelvir and for 2 weeks after the last dose.
Ensitrelvir has been detected in the milk of lactating rats. Breastfeeding should be avoided during treatment with ensitrelvir and for 2 weeks after the last dose.
DOSAGE, ADMINISTRATION, AND COST — Xocova is supplied in 125-mg tablets. The recommended dosage for postexposure prophylaxis is 375 mg on day 1, followed by 125 mg on days 2-5. Treatment should be started as soon as possible and within 72 hours of exposure to an individual infected with SARS-CoV-2. According to the manufacturer, a 5-day course of Xocova costs $1400.
CONCLUSION — The oral antiviral drug ensitrelvir (Xocova) reduces the risk of COVID-19 in household contacts of an individual infected with SARS-CoV-2. The drug is expensive, has the potential to interact with many other drugs, and should not be taken by women who are pregnant or breastfeeding.
- M Lin et al. Molecular mechanism of ensitrelvir inhibiting SARS-CoV-2 main protease and its variants. Commun Biol 2023; 6:694. doi:10.1038/s42003-023-05071-y
- Y Unoh et al. Discovery of S-217622, a noncovalent oral SARS-CoV-2 3CL protease inhibitor clinical candidate for treating COVID-19. J Med Chem 2022; 65:6499. doi:10.1021/acs.jmedchem.2c00117
- T Uehara et al. Ensitrelvir treatment-emergent amino acid substitutions in SARS-CoV-2 3CLpro detected in the SCORPIO-SR phase 3 trial. Antiviral Res 2025; 236:106097. doi:10.1016/j.antiviral.2025.106097
- FG Hayden et al. Ensitrelvir for COVID-19 postexposure prophylaxis in household contacts. N Engl J Med 2026; 394:1905. doi:10.1056/nejmoa2509306
- H Yotsuyanagi et al. Efficacy and safety of 5-day oral ensitrelvir for patients with mild to moderate COVID-19: the SCORPIO-SR randomized clinical trial. JAMA Netw Open 2024; 7:e2423203. doi:10.1001/jamanetworkopen.2023.54991
- AF Luetkemeyer et al. Ensitrelvir for the treatment of nonhospitalized adults with COVID-19: results from the SCORPIO-HR, phase 3, randomized, double-blind, placebo-controlled trial. Clin Infect Dis 2025; 80:1235. doi:10.1093/cid/ciaf029
- Inhibitors and inducers of CYP enzymes, P-glycoprotein, and other transporters. Med Lett Drugs Ther 2023 January 25 (epub). Available at: www.medicalletter.org/downloads/CYP_PGP_Tables.pdf.